- Locations
- Find a Physician
- By Physician
- By Department
- The Center for Spine Health
- Hand & Wrist Center
- Shoulder & Elbow Center
- Foot & Ankle Center
- Joint Replacement Center
- The Sports Medicine Center
- Pediatric Orthopedic Center
- Trauma & Fracture Center
- Osteoporosis and Bone Health
- Oncology Center
- Cartilage Repair Center
- Concussion Rehab Center
- OrthoDirect
- Careers
- Patient Portal
- Intranet
 Overview
Overview
Hand and wrist fractures are fairly common. Treatment depends on the severity of the fracture, whether joints are involved, location of the injury, deformity or displacement.
Children's bones are in a state of continued growth and are susceptible to fractures involving the growth plate areas. Growth plate injuries are difficult to diagnose because they do not show up on X-rays.
Fractures that require immobilization are often splinted to prevent compression injuries from a cast that covers the entire area. After an injured area is splinted, if the patient sees color change, experiences numbness, or has feeling of tightness, they should return to the medical center immediately.
Serious burn injuries will require multiple operations and skin grafting to ensure the best outcome.
All hand injuries will require close up evaluation and treatment.
Seymour Fractures
Seymour fracture is a fracture of the distal phalanx that is “open” through a nail bed laceration. Seymour fractures usually happen from a crush injury during contact sports or play. The joint nearest the end of the finger is hurt as well as the nail. Treatment for Seymour fractures includes removal of the nail along with appropriate nailbed repair, thorough fracture debridement and fracture reduction.
Our Hand and Upper Extremity Program expertly cares for children with fractures.
Open Fracture
A compound fracture, sometimes called an open fracture, is a break or open wound in the skin near the site of the fractured bone. If a bone fractures and becomes displaced, tissue can become trapped within the growth plate. The growth plate is the weakest part of a bone. Compound fractures are at a high risk for infection since the skin was broken open.
Bony Mallet Fractures
A mallet fracture occurs when the extensor tendon causes avulsion of the distal phalanx. Bony mallet fractures are more prevalent in children than adults. Bony mallet fractures in children tend to be bony avulsions of the epiphysis. Extension splinting provides excellent return of function and bony remodeling. For younger patients, splinting compliance may be an issue, and so other options such as placing a long arm cast over the splint or percutaneous pinning may be necessary.
Phalangeal Neck Fractures
 Phalangeal neck fractures (finger breaks) often happen because of a direct hit to a finger. These finger breaks or fractures are relatively uncommon and are almost exclusively seen in children. Hand and finger breaks are among the top five most common fractures that occur in childhood. Displaced and unstable phalangeal neck fractures are generally managed by closed reduction and Kirschner wire fixation. Phalangeal neck fractures have limited remodeling potential and are therefore generally treated with percutaneous bone pinning. Most pediatric hand fractures are treated conservatively.
Phalangeal neck fractures (finger breaks) often happen because of a direct hit to a finger. These finger breaks or fractures are relatively uncommon and are almost exclusively seen in children. Hand and finger breaks are among the top five most common fractures that occur in childhood. Displaced and unstable phalangeal neck fractures are generally managed by closed reduction and Kirschner wire fixation. Phalangeal neck fractures have limited remodeling potential and are therefore generally treated with percutaneous bone pinning. Most pediatric hand fractures are treated conservatively.
Some phalangeal neck or hand fractures can be difficult to identify on X-rays. These fractures have a high likelihood of displacement and a low potential for bone remodeling. These fractures occur 10x the frequency in children than adults. Phalangeal neck and hand fractures are best managed when the problem is recognized at the time of injury. Non-displaced fractures can be treated with cast immobilization. Displaced fractures are usually treated with closed reduction and pinning. It is important to watch for signs of infection during the recovery period.

Do you Need an Appointment?
We have made it easier to schedule appointments, click the button to fill out an online appointment request form or call our new central scheduling line 401-457-1500 to schedule an appointment.
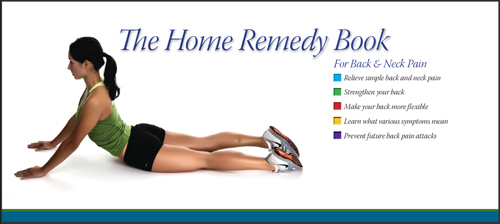
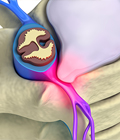
Home Remedy Book
Have back or neck pain? Learn what causes symptoms and the home remedies that relieve pain. University Orthopedics mails out Home Remedy Books to residents throughout the New England area.