- Locations
- Find a Physician
- By Physician
- By Department
- The Center for Spine Health
- Hand & Wrist Center
- Shoulder & Elbow Center
- Foot & Ankle Center
- Joint Replacement Center
- The Sports Medicine Center
- Pediatric Orthopedic Center
- Trauma & Fracture Center
- Osteoporosis and Bone Health
- Oncology Center
- Cartilage Repair Center
- Concussion Rehab Center
- OrthoDirect
- Careers
- Patient Portal
- Intranet
Flatback Syndrome | Pediatric Scoliosis | Adult Scoliosis | Surgical Options | Harrington Rod | Lordosis
 Pediatric Scoliosis
Pediatric Scoliosis
When scoliosis is present before the age of 3, this is known as Infantile Scoliosis. When scoliosis is diagnosed between the ages of 3 to 10, this is known as Juvenile Scoliosis.
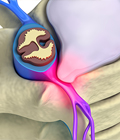
Congenital scoliosis is a condition where there is defor mity in the spine present at birth, but will usually only be discovered as the baby continues to grow. Some of the reasons causing this type of scoliosis are abnormally shaped or fused bones in the spine that do not grow or fuse correctly. Neuromuscular scoliosis consists of poor neurologic or muscular control of the spine and might be evident in a child born with cerebral palsy and muscular dystrophy. Children diagnosed with more advanced scoliosis can often feel like they sometimes have trouble breathing and experience back/leg pain among other issues.
mity in the spine present at birth, but will usually only be discovered as the baby continues to grow. Some of the reasons causing this type of scoliosis are abnormally shaped or fused bones in the spine that do not grow or fuse correctly. Neuromuscular scoliosis consists of poor neurologic or muscular control of the spine and might be evident in a child born with cerebral palsy and muscular dystrophy. Children diagnosed with more advanced scoliosis can often feel like they sometimes have trouble breathing and experience back/leg pain among other issues.
Most kids with non-severe scoliosis will not experience the painful symptoms that are often associated with scoliosis. Kids will usually be diagnosed either at a school screening being performed on the entire grade or by their doctor. Children with detectable scoliosis can appear to have a hump, “S” shaped curve in their spine, and perhaps uneven shoulders and hips while doing the Adams Forward Bending test. School examiners will inform the parent if they believe scoliosis might be present or could develop in their child. If scoliosis is discovered, it is important to see a scoliosis specialists to better evaluate the child and the doctor might take an X-ray for a better analysis. On an X-ray, the doctor uses the Cobb angle method to measure the angulations between the curving of the vertebrae.
The potential for the curvature in the spine to worsen correlates with the amount of growth remaining in the bones and spine. The amount of growth the child has left to complete is directly related to the amount and type of treatment he or she will receive since the ‘growth spurt’ years tends to make the scoliosis worse. One of the ways to measure how much growth the patient has left to complete is by taking a radiographic measure of the maturity of the pelvic bone. The Risser sign can be tracked on the pelvic X-ray to better determine if the person has more growing left to complete. The changes of puberty in girls and boys can also give insight if the person has more growing left as well. In girls, evidence suggests that the beginning of the menstrual period estimates 1.5 to 2 years of spine growth remain.
Types of Pediatric Scoliosis
Pediatric scoliosis refers to the development of a spinal curvature in children or adolescents who are still growing. There are different types of pediatric scoliosis, which can be classified based on the age of onset, cause, and specific characteristics of the spinal curvature. Here are some common types:
-
Idiopathic scoliosis: Idiopathic scoliosis is the most common type of scoliosis in children and adolescents. It refers to cases where the cause of the curvature is unknown. Idiopathic scoliosis can be further classified based on the age of onset:
a. Infantile idiopathic scoliosis: This type of scoliosis occurs in children younger than 3 years old. b. Juvenile idiopathic scoliosis: Juvenile idiopathic scoliosis develops between the ages of 3 and 10 years. c. Adolescent idiopathic scoliosis: Adolescent idiopathic scoliosis is diagnosed in individuals between the ages of 10 and 18 years.
-
Congenital scoliosis: Congenital scoliosis is present at birth and results from abnormal spinal development in the womb. It occurs due to vertebral anomalies or fusion of the vertebrae. Congenital scoliosis can vary in severity and may be associated with other congenital abnormalities or syndromes.
-
Neuromuscular scoliosis: Neuromuscular scoliosis is associated with underlying neuromuscular conditions that affect the muscles, nerves, or both. These conditions can include cerebral palsy, muscular dystrophy, spina bifida, spinal muscular atrophy, and other neuromuscular disorders. The abnormal muscle tone or weakness in these conditions can lead to imbalances and progressive spinal curvature.
-
Syndromic scoliosis: Syndromic scoliosis is a type of scoliosis that occurs as part of a genetic or chromosomal syndrome. Examples of syndromes associated with scoliosis include Marfan syndrome, Ehlers-Danlos syndrome, Down syndrome, and Prader-Willi syndrome. Children with syndromic scoliosis may have additional health issues and require specialized care.
-
Early-onset scoliosis: Early-onset scoliosis (EOS) refers to scoliosis that is diagnosed before the age of 5. It includes infantile idiopathic scoliosis, congenital scoliosis, and some cases of neuromuscular scoliosis. EOS requires early monitoring and intervention due to the potential for rapid progression and associated complications.
Each type of pediatric scoliosis requires careful evaluation and management based on the individual's age, growth potential, severity of the curvature, associated symptoms, and underlying cause. Treatment options for pediatric scoliosis can include observation, bracing, physical therapy, and, in some cases, surgery. A healthcare professional specializing in pediatric orthopedics or spine conditions can provide an accurate diagnosis and recommend appropriate treatment options based on the specific type of pediatric scoliosis and individual circumstances.
 Bracing
Bracing
Bracing is designed to apply pressure to the trunk and pelvis, which improves the alignment of the spine and allows the spine to grow in a straighter fashion. Some doctors might recommend bracing if the scoliosis starts to pass 20 degrees measured laterally in the curve. Most doctors will recommend bracing for patients with a curvature angle around 20-50 degrees. Bracing is not designed to reverse the curvature, but rather to prevent the spine from increasing the angle of the curve. They are many different types of bracing options available with specially placed padding and straps that place resistance on the certain area in the spine. Most braces are constructed of plastic and contoured to your unique body and your doctor will help prescribe which brace is best for your treatment.
The Boston Brace is probably the most common used to treat scoliosis. These braces are made out of plastic components that are custom modeled to the patients body which creates a low-profile for the brace. On the front side, this brace extends from the lower breast to the start of the pelvic area. On the back side it extends from the upper back to the tail bone. This brace forces the lower back to flex which pushes the abdomen and helps flatten the curvature in the spine.
Although surgery can be risky and expensive, it might be an avenue to consider if severe scoliosis develops with a degree angle above 40 degrees and bracing has shown no signs of stopping the spine from continually to curve. 
Children that don’t need bracing or surgery will still need to be under observation from the doctor to be aware if the spine continues to curve. The child will most likely be advised to come back for a couple follow up visits to make sure the scoliosis is not progressing into a serve curve. X-rays might be done semi-annually to make sure the curve does not worsen. Most of the time X-rays are conducted until the child stops growing or until the curving of the spine stops.
The majority of children diagnosed with scoliosis will not need any type of treatment. Less than 15% of children and adolescents diagnosed with some degree of scoliosis will actually need to begin some type of treatment including bracing and/or surgery.
There are not any specialized exercises that have been proven to help stop scoliosis. Most scoliosis in children should not prevent them from enjoying time with friends or playing sports.



Do you Need an Appointment?
We have made it easier to schedule appointments, click the button to fill out an online appointment request form or call our new central scheduling line 401-457-1500 to schedule an appointment.
Home Remedy Book
Have back or neck pain? Learn what causes symptoms and the home remedies that relieve pain. University Orthopedics mails out Home Remedy Books to residents throughout the New England area.