- Locations
- Find a Physician
- By Physician
- By Department
- The Center for Spine Health
- Hand & Wrist Center
- Shoulder & Elbow Center
- Foot & Ankle Center
- Joint Replacement Center
- The Sports Medicine Center
- Pediatric Orthopedic Center
- Trauma & Fracture Center
- Osteoporosis and Bone Health
- Oncology Center
- Cartilage Repair Center
- Concussion Rehab Center
- OrthoDirect
- Careers
- Patient Portal
- Intranet
Surgical Options - Spine
- Minimally Invasive Spine Surgery Overview
- MIS ALIF: Anterior Lumbar Interbody Fusion
- MIS AxiaLIF: Presacral Lumbar Interbody Fusion
- MIS ILIF: Interlaminar Lumbar Instrumented Fusion
- MIS: Microdiscectomy
- MIS PLIF: Posterior Lumbar Interbody Fusion
- MIS TLIF: Transforaminal Lumbar Interbody Fusion
- MIS XLIF: Extreme Lateral Interbody Fusion
Studies show that more than half of back surgeries are unnecessary and the goal of University Orthopedics is to exhaust nonsurgical treatment for spine problems before using spine surgery. There are times when surgery is the best treatment for a spine condition. The fellowship-trained spine surgeons at University Orthopedics are proficient in the latest spine surgery techniques and procedures. Some of the common spine procedures performed by our spine surgery specialists include minimally invasive spine surgery, microdiscectomy and spine fusions.
Common Back Surgeries:
Lumbar Discectomy | Cervical
Discectomy | Spinal Fusion | Laminectomy | Rhizotomy | Scoliosis
Surgery | Dorsal Column Stimulation
Lumbar Discectomy
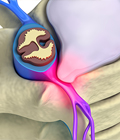
Discectomy is the removal of the herniated portion of a disc to relieve the pressure on nearby nerves as they exit the spinal canal. Contrary to myths, the disc does not slip out of position like a watermelon seed. Instead, the disc is like a jelly donut, acting as the functional shock absorber between two bony vertebrae.
An injury, or damage from a lifting incident, may cause the jelly center to break through the wall of the disc. When the disc herniates, the jelly center can press on nearby nerves. This causes back or leg pain when the herniation is in the low back, and arm pain if the disc is in the neck area.
In a lumbar discectomy, the surgeon typically only removes the portion of the disc that is causing a problem, not the entire disc. If you have a herniated disc, keep in mind that a disc has a purpose. When you remove a disc, it may cause instability in the joint, and a surgeon may recommend a fusion to re-stabilize the area.
The surgeon can remove the damaged piece of disc through a traditional incision in the back or neck or with a surgical probe, such as in percutaneous discectomy.
Depending on the nature of your disc problem, your surgeon will recommend
the most appropriate type of surgery for you.
[Top]
Cervical Discectomy
Cervical is the medical term for "neck." Just as in a lumbar
discectomy, the surgeon will remove a piece of damaged disc tissue in
the neck area to relieve pressure on the spinal cord or nerve roots.
In some cases, by removing a piece of the shock-absorbing disc that separates
the two vertebrae, the structures may become less stable. Consequently,
when the disc is removed, a surgeon may recommend "fusing" the
vertebrae to prevent instability. This fusion surgery may require a second
incision in the front of the neck to gain access to the disc area. A
cervical discectomy is best left to surgeons who specialize in spine.
[Top]
Spinal Fusion
A surgeon may use bone from the patient's hip or from a bone bank to stabilize two vertebrae after a discectomy. During a fusion surgery, the disc is removed, and the surgeon inserts a small wedge of bone in between the two vertebrae to restore the disc space. Over time, the two vertebrae "fuse" together into a solid structure. While this limits movement and flexibility, it can also help to ease pain.
The decision to fuse or not to fuse can be a complex one.
It will probably be based on the surgeon's assessment of two factors:
the amount of instability that a discectomy will cause and how much disc
space is necessary to restore. If the surgeon opts not to do a fusion,
a different follow-up surgery may be recommended.
[Top]
Laminectomy
A laminectomy involves the removal of part or all of the bone covering
the spinal canal. The purpose of this procedure can be to free nerve
roots, remove a tumor, bone spur or to perform certain types of fusion
procedures.
Removing the lamina (laminectomy) is much like removing the cover on a fuse box to access the wiring. By removing the lamina, the surgeon gains access to the disc area and frees more space for the nerves inside.
During the surgery, a one to two-inch incision is made in the low back. The spine surgeon then chips away the lamina of one or more vertebrae to gain access to the disc area. The surgeon will then remove any fragments that may have broken away from the disc, as well as the area of disc that is herniated and pressuring a nerve root. The entire disc is not removed. If it was, you would lose the shock-absorbing function of the disc between the vertebrae. Instead, the surgeon typically removes the part of the disc that has ruptured outward, along with another 10 or 20 percent of the disc, in order to prevent future problems from arising.
A laminectomy is often used to treat recurrent disc
herniations, or where scar tissue is involved. Laminectomy may
also be used in cases of spinal stenosis in which the entire canal
is narrowed like a ring on a swollen finger.
[Top]
Rhizotomy
Rhizotomy is a procedure in which the physician may use heat or cold to intentionally damage the ability of a problematic nerve to telegraph pain signals to the brain. While pain signals serve to warn us about danger or injury, sometimes a nerve can end up in a "stuck" position, sending a continuous pain signal to the brain.

"Neuroablation" is another word used to describe the surgical procedure to purposely inhibit the nerve's ability to transmit a pain signal. During the procedure, the spine surgeon can destroy the problematic nerve by cutting it or by using extreme heat or cold. This intentional "short circuit" can be temporary or permanent, depending upon the procedure.
Trying to mask this signal with drugs can have damaging
long-term implications. Drugs can have dangerous side effects to internal
organs. By using rhizotomy, the pain signal is turned off at the source.
[Top]
Scoliosis Surgery
Through the placement of hooks, rods and screws, a spinal curve can be corrected and stabilized. A fusion often follows scoliosis surgery, in order to maintain the correction permanently.
Scoliosis is not the result of an injury and usually appears without cause. It can be inherited, and it usually affects more women than men. In the case of most spinal curves, the spine is not only bent but twisted like a bent corkscrew.
Some cases of scoliosis are not serious. Over time, if a curve worsens, surgery may be required to correct the curve. In extreme cases, if the curve is not corrected, the spinal deformity can place pressure on internal organs, which can shorten a person's life expectancy.
During scoliosis surgery, the surgeon may use special instruments
that hook onto various vertebra segments. These surgical rods are the
adjusted to "de-rotate" the twisted and bent corkscrew.
Decades ago, Harrington Rods were used to surgically straighten the spine. However, this technique did not untwist or correct the spine. Current state-of-the-art instrumentation achieves much better spine correction than older rods did.
Generally speaking, the younger the patient, the more flexible the spine and the better the result from scoliosis surgery. As the patient becomes older, say over 40 years old, the spine is less flexible, and there may be a greater risk involved in attempting to correct the curve. Because the spinal cord is involved, only spine surgeons who specialize in scoliosis should perform scoliosis surgery.
Dorsal Column Stimulation
Dorsal column stimulation, also known as spinal cord stimulation, is used in complex cases of back pain that cannot be resolved nonsurgically or with another surgery. In most cases, it is used when leg pain is worse than back pain. The intent of dorsal column stimulation is to use an electrical signal, instead of drugs, to mask pain that cannot be removed any other way.
During this procedure, the patient is awake, and the surgeon
delicately places tiny electrodes under the skin in the back. At that
point, a tiny electrical current is transmitted through the wires to
the desired location in the back. This sensation feels like a tiny tickle,
as the electrical current interrupts the pain signal that may be sent
to the brain from the damaged nerve. The patient helps instruct the surgeon
as to which electrical setting and placement of wires produces the most
pain relief. It is important to note that this technique is only used
in the most extreme cases of back and leg pain.
[Top]

Do you Need an Appointment?
We have made it easier to schedule appointments, click the button to fill out an online appointment request form or call our new central scheduling line 401-457-1500 to schedule an appointment.
Home Remedy Book
Have back or neck pain? Learn what causes symptoms and the home remedies that relieve pain. University Orthopedics mails out Home Remedy Books to residents throughout the New England area.