- Locations
- Find a Physician
- By Physician
- By Department
- The Center for Spine Health
- Hand & Wrist Center
- Shoulder & Elbow Center
- Foot & Ankle Center
- Joint Replacement Center
- The Sports Medicine Center
- Pediatric Orthopedic Center
- Trauma & Fracture Center
- Osteoporosis and Bone Health
- Oncology Center
- Cartilage Repair Center
- Concussion Rehab Center
- OrthoDirect
- Careers
- Patient Portal
- Intranet
 Overview
Overview
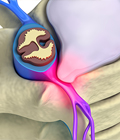
Nerve reconstructive options include allograft and autograft nerve grafts, nerve transfers and nerve conduits to bridge digital sensory nerve gaps. The gold standard in nerve repair is primary end-to-end coaptation.
If damage to the nerve occurs too far away from the affected muscles, recovery is not possible with just nerve repair surgery.
Reconstruction procedures to restore lost function include tendon transfers that takes working muscles that are adjacent to a paralyzed muscle, and substituting the movement of one muscle for another by reconnecting the tendons from the uninjured muscle to the injured one. The new movement from the transferred muscle maximizes function in that specific area.
Nerve Reconstruction
Nerve reconstruction is the term given to the various microsurgical techniques used to treat nerve injury. Early intervention is extremely important for obtaining a positive outcome. For the best results, nerve reconstruction should begin between 3-6 months after the injury.
Primary nerve reconstruction are optimally performed 3-6 months after injury.
Secondary reconstructive procedures include tendon transfers, free muscle transplants, pedicle muscle transfers, and fusions. These secondary procedures can often be done months or years after the injury.
Recovery
Recovery from reconstructive nerve surgery is a lengthy process. Long-term physical therapy helps to preserve range of motion, strength, and flexibility in the affected area. Physical therapy also helps muscle atrophy.
[Top]

Do you Need an Appointment?
We have made it easier to schedule appointments, click the button to fill out an online appointment request form or call our new central scheduling line 401-457-1500 to schedule an appointment.
Home Remedy Book
Have back or neck pain? Learn what causes symptoms and the home remedies that relieve pain. University Orthopedics mails out Home Remedy Books to residents throughout the New England area.